| ESE504 : The Class : Advanced CD : Hearing disability | |||||
As each of us gets older, we lose some of our hearing. Some of the loss comes from exposure to unacceptable noise bombardment, some from taking medications, some from the aging of the mechanisms of the ear. Most of us do not think of ourselves as hard of hearing. In fact, we may fail to realize that we have lost hearing ability until it becomes quite pronounced.
This helps explain why it is difficult for parents and children to recognize a hearing impairment. Of course, we are much more aware of deafness, but being unable to hear, or having a profound hearing loss is quite rare, while having a hearing impairment is much more common.
|
|
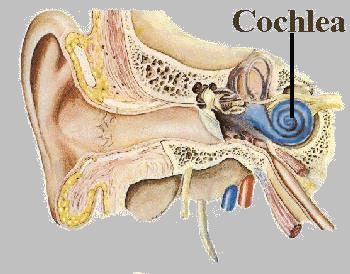
Sound is collected in the outer ear, travels through the ossicles (or bones) of the middle ear and delivers pressure waves through the oval window of the cochlea (of the inner ear) onto the basilar membrane. The inner ear is a fluid-filled space. The cochlea contains sensory cells that are set off by auditory stimuli. The vestibular system contains sensory cells that are sensitive to rotational motion, linear motion, and changes in the position of the head with respect to the ground. |
So, how does this work to create hearing? More graphic representations? Click here.
|
|
. Both the external ear and middle ear are air-filled spaces. The key work of the external ear and middle ear is to convert air pressure waves into liquid pressure waves. "Air pressure waves" are "sound waves." Liquid pressure waves in the inner ear stimulate highly-specialized nerve cells in the cochlea. Then nerve impulses are sent to the brain, and the mind perceives sound - HEARS. |
![]()
Hearing loss is described as either conductive (the flow of energy down to the cochlea) or sensorineural ("sensory" refers to the nerve cells in the cochlea which "fire" in response to the fluid pressure wave; "neural" refers to nerve impulses beginning with the auditory nerve, which exits the cochlea and enters the brainstem, and all other nerves within the brain ultimately leading to the auditory cortex.)
CONDUCTIVE HEARING LOSS: This term is used when there are problems which the flow of air pressure waves down the ear canal, across the ear drum, or through the ossicles. Some examples of problems that cause conductive hearing loss: wax impaction in the canal, infection in the canal, causing the canal to swell shut, infection, scarring or perforation of the ear drum. disruption of the ossicles fluid in the middle ear space impaired mobility of the ossicles.
If the ossicles can't vibrate, sound waves cannot very well be transmitted through them. Chronic infection can cause scars or adhesions to impair the mobility of the ossicles. In a condition known as otosclerosis, the stapes becomes "frozen in place" by bony scarring.
SENSORINEURAL HEARING LOSS. ![]() Drug-induced damage of the cochlea (examples: antibiotics such as gentamicin;
chemotherapy drugs, such as cisplatin.)
Drug-induced damage of the cochlea (examples: antibiotics such as gentamicin;
chemotherapy drugs, such as cisplatin.) ![]() Traumatic damage of the cochlea (noise is a form of trauma; a blow to
the head, or penetrating injury of the inner ear, can also cause sensorineural
hearing loss.)
Traumatic damage of the cochlea (noise is a form of trauma; a blow to
the head, or penetrating injury of the inner ear, can also cause sensorineural
hearing loss.) ![]() Age-related damage of the cochlea (presbyacusis.)
Age-related damage of the cochlea (presbyacusis.)![]() A tumor on the auditory nerve (acoustic neuroma or schwannoma.)
A tumor on the auditory nerve (acoustic neuroma or schwannoma.) ![]() Certain infections, such as meningitis.
Certain infections, such as meningitis.
 |
Click here to visit a site on a neonatal hearing test |
|
Adapted from a paper on identifying hearing losses in new borns - Amie L. Gordon-Langbein, D.O.* Hearing loss in children is high. Studies suggest that 14.9 percent of school-aged children have some degree of hearing loss .Out of 1000 newborns, 3 to 6 are born with congenital bilateral sensorineural hearing loss. So, congenital hearing loss is one of the most common health conditions to affect newborn babies today. It is more common than any other health condition newborns are currently screened for by means of blood samples. Unfortunately, the average age for detecting a congenital hearing loss in the US is two-and-a-half years. Children with mild to moderate hearing loss tend to be diagnosed even later, at age four. A baby cannot usually tell that he or she cannot hear. Hearing loss is invisible! since the child does not realize that others hear more than they can, they are unlikely to tell anyone of hearing problems. Any degree of hearing loss is significant in a young child since hearing loss can affect children's behavior, self-esteem, and academic performance, as well as their social interactions with others. After all, hearing is fundamental to learning language, especially in children, who have yet to master the basic building blocks of speaking. Studies estimate that as much as 90 percent of what young children learn comes through reception of incidental conversations around them. To acquire new information, children must be able to hear the information, and through a series of complex events send the information to their brains for further processing. The first four years of a child's life are crucial in terms of speech and language development, and clearly speech and language skills are the precursors to higher levels of cognitive maturation. Researchers have postulated that 80 percent of a child's ability to acquire speech, language, and other cognitive processes is determined by the time they are three years of age (ASHA, 1997). Children who cannot hear the world around them are at a distinct disadvantage on a multitude of levels. Early detection of hearing loss is the key to early intervention. Researcher Christine Yoshinago-Itano has demonstrated that if a newborn with a hearing loss is diagnosed prior to six months of age and treated appropriately, the child achieves higher language levels than children with delayed diagnoses (Yoshinago-Itano, Sedey, Coulter, and Mehl, 1998). Likewise, children who are diagnosed and treated early develop speech and language skills equivalent to their peers (Yoshinaga-Itano et al., 1998). References American Academy of Pediatrics, Task Force on Newborn and Infant Hearing. (1999). Newborn and infant hearing loss: Detection and intervention. Pediatrics,103, 527-530. American-Speech-Language-Hearing Association. (1991). Joint Committee on Infant Hearing 1990 Position Statement, 22(Suppl. 5), 3-6. American Speech-Language-Hearing Association. (1997). Model Universal Newborn/Infant Hearing Screening, Tracking, and Intervention Bill, 1-10. Anderson, K. L. (1992). Keys to effective hearing conservation programs: Hearing status of school age children. In E. Cherow (Ed.), Proceedings of the ASHA Audiology Superconference (pp. 38-47). Bess, F. H., & Paradise, J. L. (1994). Universal screening for infant hearing impairment: Not simple, not risk-free, not necessarily beneficial and not presently justified. Pediatrics, 93, 330-334. Flexer, C. (1993, August 14). Classroom management of children with hearing loss: Preferential seating is not enough. Presentation, San Francisco, CA. Mehl, A. L., & Thomson V. (1998). Newborn hearing screening: The great omission. Pediatrics,101, E4. Musselman, C. R., Wilson, A. K., & Lindsay, P. H. (1988). Effects of early intervention on hearing impaired children. Exceptional Children, 55, 222-228. National Institutes of Health Consensus Statement. (1993, March). Early identification of hearing impairment in infants and young children. National Institutes of Health Consensus Development Statement, Bethesda, MD, 1-24. Niskar, A. S., Kieszak, S. M., Holmes, A., Estaban, E., Rubin, C., Brody, D. J. (1998). Prevalence of hearing loss among children 6-19 years of age: The third national health and nutrition examination survey. Journal of the American Medical Association, 279(14), 1071-1075. Northern, J. L., & Downs, M. P. (1991). Hearing in children, 4th edition. Baltimore, MD: Williams & Wilkins. White, K. R., Vohr, B. R. & Behrens, T. R. (1993). Universal newborn hearing screening using transient evoked otoacoustic emissions: Results of the Rhode Island Hearing Assessment Project. Seminars in Hearing,14, 18-29. Yoshinago-Itano, C., Sedey, A. L., Coulter, D. K., & Mehl, A. L. (1998). Early- and later-identified children with hearing loss. Pediatrics,102, 1161-1171. * Amie L. Gordon-Langbein, D.O., is a parent of two children, one of whom has a hearing loss. She is also a board-certified family physician and works as a consultant and advocate for children with hearing loss and their families. She is a member of the Alexander Graham Bell Association for the Deaf and Hard of Hearing. - http://www.agbell.org/langbein.html |
Fill out this chart to clarify the differences in the two major types of hearing loss: [25 points].
| Type of Loss | Where located | How to assess it | How to correct it | Instructional ideas |
| Conductive | ||||
| Sensorineural |
![]()
|
Potential Causes of Hearing Loss
|
|
Viral infections like mumps or measles Premature birth Anoxia Prenatal infections Meningitis or other bacterial infections Side effects from medicines ( including aspirin and antibiotics) Excessive noise - above 85 decibels |
![]()
|
Subject
|
Personal notes
|
|
Hearing disorders home page National Institute of Health (NIH) info on early recognition of hearing loss Article on early screening Links to support and strategies for hearing Links on international sites Center to facilitate children hearing Explanation of biological components of the ear Listen up web site with activities, exercises, readings, and more |
![]()
|
Deafness does not prevent language acquisition! |
|
Jennifer Woolensack Kent State University Gaines, R., & Halpern-Felsher, B. L. (1995). Language preference and communication development of a hearing and deaf twin pair. American Annals of the Deaf, 140(1), 47-55. Summary: Language characteristics of deaf and hard of hearing students vary as all children's characteristics do. However, language and communication development can be enhanced by preference and environmental factors. The twins being studied are both girls, one is Ann, who was healthy until the age of 7 months, when she contracted pneumococcal meningitis and became binaurally profoundly deaf. The other twin is Dianne, who is hearing and healthy. The study examines the communication development and language preferences of twin girls who are alike in age, genetic structure, and home and school environment, but who are different in one particular way: hearing ability. At the age of 13 months, the twins were brought to HI CHIPS program, to educate them both at the same place. They were taught both vocal and sign language. The twins were videotaped over a 20-month period, in monthly intervals. All communication was recorded and categorized by style. The language preference analysis showed that Ann preferred nonvocal language, and that Diane used vocal language. The bulk of the hand gestures were used in the request category by both twins. However, body movements were preferred much more by Ann. The study showed that both twins had the ability to learn language and to communicate. This shows that deafness does not prevent language acquisition. Although Ann was not as successful in vocal language, she still was able to develop appropriate visual language that was parallel to her chronological age. Diane was able to use both forms of language, visual and vocal, but preferred vocal. However, with knowing both forms, she helped her twin sister by communicating with her, which made Ann's language development more accelerated. This observation shows that early intervention and diverse modes of communication can benefit the development of language, especially for the deaf. Key Points: Language characteristics vary from person to person, but environment and preference play a crucial role. Deafness does not prevent language acquisition. Early intervention and diverse communication are key to the development of language for the deaf. |
 Information
Information![]()
 Tips and Strategies on Using Technology
Tips and Strategies on Using Technology
|
Educational
Interventions
|
Applications
|
Links
|
Critique
|
|
Assistive Listening Devices
|
|||
| Telecommunication Devices | |||
| Computerized Speech-to-text Translations | |||
|
Alerting devices |
|||
| Other | |||
| Cochlear Implants |
Summarize what each of these applications offers to those who are hearing impaired. In addition, find five links for each of these technological advances. Feel free to add a critique on the pros and cons or feelings of those who have utilized them [50 points].
Portraits of Helen Keller using various forms of communication with Alexander Graham Bell
|
Hearing loss
may be misunderstood and can be something missed in initial observations.
Be certain to check hearing as one of the first procedures --
and if there is a possibility of inner ear infections, continue
to monitor hearing as a potential contributor to communication
disorders.
|
|
|
Characteristics that suggest a closer look
at the possibility of a hearing impairment
|
|
| Communications | Poor speech, limited vocabulary, voice quality is poor - tone, strained sound, unusually high |
| Social functioning | Withdrawn behaviors, dependent on teacher, difficulty making friends, less socially mature, may be quite irritable or angry |
| Academic | Achievement is below ability, limited written language, spelling is unusual, as though missing sounds or hearing things others do not hear, phonetic instruction changes verbalizations |
| Hearing function | Does not seem to respond to verbal instructions, may not come when bell rings, seems to lip read when communicating |
Picture array of Helen Keller with different celebrities
|
American Sign Language For many years -- certainly long before anyone reading this was born, a deaf culture has existed. Children could find support, education and companionship among others who spoke through signs. The deaf culture protected and cared for individuals and gave them a sense of identity and acceptance long before PL94-142. You can learn to sign by using some of these locations on the web. There are also commercial CDs available that show people signing. Not only does this help in the work with youngsters who cannot hear, it is a powerful tool to use when a youngster has an auditory processing deficit. In fact, I find that a sign is a better tool in working with some youngsters who are mentally retarded, as well, since it speeds up processing time and they enjoy the physical motions and nonverbal cueing. Seriously consider giving yourself and others the gift of learning to sign. |
![]()
A Big Debate
There are four basic approaches that are currently used with children who are hard of hearing, or deaf. Some people have very strong feelings about one way or another being the "BEST" or "ONLY" way to teach students. For some reason, any time we are talking about the long and difficult practice of teaching communication skills, we get heavy investment -- like the so-called reading wars - phonics or whole language, short vowels or long vowels first, basals or language experience. Some of the discussions are intercontinental, even.
The feelings can be very strong about the approach used to support children with hearing losses. In part, it comes from the fact that each approach is successful with some students -- and each approach has been used to help students who were failing when using some other way to learn to communicate. Perhaps some also comes from the length of time that a deaf community has existed and the strong family feeling that can come from feeling "at home" with someone who can share our own feelings, break the sense of isolation.
Something to ponder -- can we read minds? Can you tell what the person sitting next to you thinks or feels? No! Even when we are in community - grow up with a mother, father, grandparent, sibling, we are not able to break out of the isolation of being the only one who really feels our own headache, depression, misery.
At least we can talk about it with others, and the talking soothes us, helps us feel that we are not alone.
Now imagine a child growing up without that facility - not really able to slip into language and share feelings, ideas, frustrations without adding to the frustration by the road blocks that communicating highlights. In that place, would you look for others who could share? Would you feel anger and alienation? What if there were a simple way to share emotions, ideas and a stream of consciousness by gesturing, moving, motioning? How invested might you become in finding others, identifying with others, feeling close to others who could do the same -- who wanted to do what it took to understand you?
Well, enough supposition. Why not look at the debate yourself?
![]()
|
Students with Hearing Loss by Jill Stedman |
|
There are many things in life that we are blessed with that we take for granted. We can walk, talk, hear and see things in our world. For the most part we don�t have any huge disabilities, and we walk around assuming everyone has it just as easy. But they don�t. There are millions of Americans who get up each morning and go about a days work struggling through our world of communication. They wake up but not to the sound of an alarm clock or music, not to the voice of the ones they love, but to silence. These Americans can�t hear, and it affects the lives of about twenty million people living in the United States. Before we can totally grasp the thought of waking up to silence each morning, we must first understand how our hearing ears work and then what goes wrong with deaf peoples ears. There are three main parts to our ears and three different levels on which we hear. First, lets start with the parts of the ear. Starting with the part you can see there is the outer ear. This part of our ears doesn�t do that much, but without it there would be nothing to direct sound into the rest of our ear. So the pinna (the outer part of the ear you can see) collects sounds and directs them back into the auditory canal. It is also a protector, in that it protects the internal structures of our ears. Then we move toward the middle ear. The eardrum separates the outer ear and the middle ear. When you get past the eardrum you would see three small bones. These bones carry the vibrations of sound across the middle ear into the inner ear cavity. These bones are called the malleus, incus and stapes. There is also the Eustachian tube that sits in the middle ear and it equalizes the pressure built up in your ears. When someone gets and ear infection, it is because the Eustachian tube isn�t controlling the air pressure correctly and fluid builds up as a result. So the last part of the ear that we need to know is the inner ear. Inside there are the most important parts of our ears. There is the cochlea and the vestibular mechanism. The vestibular mechanism is used so we can keep our balance, but the cochlea is the whole reason we can hear. In its small snail shell form it contains the auditory nerve endings. Those nerve endings are what sense the sound vibrations and with the help of central auditory processing we can hear and understand speech and language. Now lets look at the different levels in which we hear. These have been studied and given to us by a man named Ramsdell. He says that we hear on a symbolic level, a signal or warning level and an auditory background or primitive level. The symbolic level is used to understand another persons spoken words. It helps us to turn the words into actual objects or concepts in our minds. The signal or warning level keeps us alert of our surroundings and whether or not we need to fear something. The auditory background or primitive level is how we monitor our surroundings constantly. For someone that is considered hard-of-hearing, they don�t have the ability to perform at the auditory background level. Now that we know something about the way we hear, let�s look at what it really means to be deaf or hearing impaired. These two words have different meanings although many people use them interchangeably.
Those that are hard of hearing generally gain this problem through aging or from the work that they do. Deafness is brought on by birth problems, illness or accident. If you were born deaf, then you would be congenitally deaf. There would be a reason behind how you developed and such; it wasn�t caused by an accident or any kind of illness. Then there is adventitious deafness. This is when someone born with normal hearing experiences nonfunctional hearing because of and accident or illness. This can last only a little while or it can be permanent. We will look at adventitiously deaf in more depth, because it has more causes and resolutions to it. The first big thing is that there are five major types of adventitiously deaf. They are 1) conductive, 2) sensorineural, 3) mixed hearing loss, 4) functional, or 5) central auditory disorder. Each type of hearing loss has some reason and some result to it. Conductive hearing loss stems from a structural problem with the outer and middle ear. The most common cause of this is otitis media, otherwise known as an ear infection. This is especially common among school age children and it can be fixed with medication. If it becomes a constant problem with a child, they may need to surgically place a special tube inside the ear to help the Eustachian tube to correctly balance the air pressure. The conductive hearing loss can also result from an earwax build-up or otoscierosis. Otoscierosis is a spongy, bony growth around the stapes one. If this occurs a doctor can do surgery to overcome the difficulty. There is rarely a time that a conductive hearing loss becomes so severe that it is permanent. For the most part, these problems can be treated and the child will have normal hearing, speech and language. A more serious form of hearing loss is sensorineural hearing loss. This occurs when damage has been done to the cochlea or the auditory nerve. A viral disease is a major one of the causes, although other illnesses and disease can cause this. It requires painstaking treatment, and cannot be cured all the way. The degree to which a child may be deaf depends. One way a baby may be born with sensorineural hearing loss is if the pregnant mother catches rubella during the first three months of pregnancy. Another big cause for babies with sensorineural problems is Rh incompatibility. Usually babies born under these circumstances don�t survive, but if they do they have a high risk of being deaf. Hereditary factors may also play in the role of hearing loss in children. Someone with mixed hearing loss has a mixture of the problems discussed above. This kind of hearing loss can create incredible difficulties for school children. The last two hearing loss problems are functional hearing loss and central auditory disorders. A functional hearing loss is usually to compensate for another problem a child is having. It is usually masking some type of real or perceived social or psychological struggle. This occurs generally in children ages of 9 to 13. These are also usually found in the hearing tests performed in schools. A central auditory disorder is one where there isn�t any measurable peripheral hearing loss. It is a result of a lesion or damage to the central nervous system. The child may show signs of difficulty with auditory comprehension, language development or auditory learning. The actual cause of this is very hard to discover. As I said in the introduction, there are millions of Americans that fight with this everyday. Total there is about 8-10 percent of people in this country with a hearing disorder of some kind. Over a million pre-school, elementary and secondary education children have hearing loss and twelve million young adults between the ages of 18 and 25. This is a very prevalent problem within the United States, and I�m sure with the rest of the world as well. As a future teacher, I know that it could affect my classroom and so it is important that I am aware, as with the rest of teachers, what signs to look for and how it affects a classroom. There are many ways to evaluate someone�s hearing ability. Most schools, if not all public schools perform a pure tone-screening test. This is when the child hears different frequencies from a machine and must raise his/her hand to respond to it. They test the frequency range from 250 Hz to 8000 Hz and at an intensity of 20 to 25 dB. Another type of test is a threshold test. There is the air conduction threshold test that will reveal any hearing loss and tells the amount as well. Then there is the bone conduction, which measures the sensorineural mechanism of the inner ear. This is the best test to check for a mixed or sensorineural hearing loss. There are also the speech reception threshold test and special audiometric test. The speech test will test whether or not a child can hear and understand speech and the special audiometric helps physicians treat otitis media, a middle ear infection. There are many types of treatments that can help make hearing loss easier on the individual. There are hearing aids and assistive listening devices that can make it easier for the deaf to make it in a communication-based world. There is also auditory training that can teach those with hearing impairment to use their residual hearing to its greatest extent. This kind of training is used to familiarize parent and children with the nature of hearing loss, with the types of rehabilitation and with what they can expect from auditory training. When educating a child with hearing loss, you must first know how to recognize the problem. One big thing to notice in a child with possible hearing loss is whether they are paying attention in class. If they have a lot of earaches or a discharge from their ear(s) it is a good idea to have them sent to a doctor. When they can�t answer easy questions or they fail to respond when spoken to it is possible that they are having trouble hearing speech and language. Teachers also need to be aware that there are specific ways to teach children with hearing loss. Those children with mild to moderate hearing loss should be given appropriate seating in the classroom and special attention to complete their work. They may need to be placed in a special class depending on how they progress through school. IF a child has moderate to severe hearing loss they will probably need special therapy and reinforced drills in the classroom. If there are more than one hearing impaired student in any particular classroom, it is advised that a teacher set up some sort of auditory training unit so they can help each other out. When it comes to social and personal concerns, there can be many problems. When a child becomes deaf at an early age or is born deaf they can have a high frequency of emotional and social adjustments. These result from parental difficulty with accepting deafness, lack of a role model, and limited activities in school and out of school. When considering the career of a teacher, you must realize that there are hurdles that you might have to jump over in the classroom. You have to be able to be flexible and work with children when they need help. Teachers need to be aware of their students� struggles and disabilities. So when thinking of having a career that will greatly impact hundreds or thousands of lives, you must be able to assess the children correctly and be able to help them if they have special needs. |
|
Communication Approach
|
Definition |
Justification
|
Pros and Cons
|
| Oral Only |
|
||
| Total communication |
|
||
| Cued speech | |||
| Bilingual-bicultural |
Fill in the chart, using the ideas you gain from reading the text and in your web searches. Try to talk with a person who is invested in one of the approaches, and if possible, talk with the parents or chums to see a more varied look at the emotions and investments surrounding this critical debate. [25 points have been allotted for this activity].
![]() Activity
List
Activity
List ![]()
1. Read a book written by a family member, telling about their personal insights and challenges. Make a list of the ways a teacher might support the parent and child experiences. Make a second list of things parents might tell an educator about a child with hearing problems. [50 points].
2. Locate a parent who will allow you to visit the child at the school or in the home and spend a minimum of 4 hours observing the youngster. As part of the observation experience, identify at least three student strengths. Look for the youngster's interests and determine some of the ways contact points that could be used to engage the student. How does the family engage the student? What adaptations are made to help the child and what adaptations does the child make to engage the family? [25 points per hour for observing; 50 points for the adaptation summary].
3. Watch The Miracle Worker, the movie for 50 points and send a review of the characterization of Helen Keller as a person without language or hearing for another 25 points.
4. Learn about the controversy in signing or speaking as part of the feelings communicated by the community. Try to find an opportunity to watch someone use signing with a child. After looking at the pros and cons, develop a paragraph stating your personal feelings about the controversy. [25 points]
5. Identify three commonly held fallacies about autism and then provide three fact based beliefs about people with hearing impairment. [15 points]
6. Locate and review one of the diagnostic instruments used to evaluate youngsters who may have a hearing loss. You may offer to help a nurse at a local school give hearing tests. Do you think the tests are accurate? Adequate?[25 points].
7. Remember to feel free to develop your own personal response to the material. Allot yourself approximately 25 points per hour for your work.
8. There are several very different kinds of hearing losses that are included in the broad diagnoses. Choose one of the categories and find at least 10 articles or discussions about the characteristics of the particular kind or level of hearing loss.. Feel free to use materials off the web, as well. Then write a paper of 500-1000 words, discussing the challenges these young people have and suggest a set of methods or materials that might address strengths and diminish barriers to education. [100 points for each paper.]
9. Go to a company, such as Beltone and have your own hearing checked. Report how it feels and the results of the assessment. [25 points].
10. Take a short course in sign language to learn to sign. Give yourself 25 points for each hour you spend learning to sign.
11. Find someone who uses ASL exclusively to communicate and interview them about the process, the strengths and weaknesses of the medium. [25 points].
12. Speak with the phone company about the TDD. Make a point of searching for a TDD phone in each building you go to for a week. [50 points].
 Book List
Book List
Bragg, Bernard. (1989). Lessons in laughter: The autobiography of a deaf actor (as signed to Eugene Bergman). Washington, DC: Gallaudet University Press. Bragg, a deaf child born to deaf parents, is Deaf, not deaf, where the capitalized letter denotes a linguistic and cultural minority. The author is an accomplished actor in deaf drama.
Cohen, Leah H. (1994). Train go sorry: Inside a deaf world. Boston: Houghton Mifflin. The author relates personal experience of deafness, focusing especially on the Lexington School during its attempt to assimilate signing into a historically oral educational tradition.
Gibson, William. (1960). The miracle worker. New York: Bantam Books. This play is based on the story of Helen Keller and her teacher, Annie Sullivan.
Groce, Nora E. (1985). Everyone here spoke sign language. Cambridge, MA: Harvard University Press. For over 200 years, Martha's Vineyard had a high incidence of people with hereditary deafness. Thus, nearly all the residents, both hearing and deaf, learned sign language. This book shares the oral history gathered from about 50 witnesses.
Keller, Helen. (1961). The story of my life: The autobiography of Helen Keller. New York: Dell Books. Keller writes her own story.
Lane, Harlan. (1984). When the mind hears: A history of the deaf. New York: Random House. This book tells about the history and culture of the deaf. American Sign Language is sponsored.
Lane, Harlan. (1992). The mask of benevolence: Disabling the deaf community. New York: Alfred A. Knopf. Lane offers a historical review of attitudes toward deaf people in Europe and America. He argues against the use of cochlear implants in children.
Merker, Hannah. (1994). Listening. New York: Harper Collins. The author who experienced a trauma induced severe hearing loss at the age of 39 discusses the various difficulties of her hearing loss, and the stigma attached to it.
Sacks, Oliver. (1991). Seeing voices: A journey into the world of the deaf. London: Pan Books. Sacks, a neurologist, turns his writing talents to understanding deaf society. He reviews the education of the deaf in America, considers American Sign Language, and Gallaudet College. He argues for ASL as the preferred language for the deaf.
Sidransky, Ruth. (1990). In silence: Growing up hearing in a deaf world. New York: St Martin's. A hearing child of deaf parents shares personal and intense feelings of straddeling two worlds.
Spradley, Thomas, & Spradley, James. (1978). Deaf like me (reprint). Washington, D.C.: Gallaudet University Press. The focus of this book is the family endeavor to bring Lynn into the world of oral communication, eventually becoming disenchanted with oralism and recognizing the importance of sign as the means to Lynn's communicative life.
Walker, Lou Ann. (1986). A loss for words: The story of deafness in a family. New York: Harper and Row. Walker shares her experiences as the hearing child of deaf parents.
Listen-up web site with book lists in several areas.
Singular Book company - large array of books on the subject
Movies
Amy
Bridge to Silence
Children of A Lesser God
Dead Silence (HBO TV-movie)
For A Deaf Son (PBS Documentary)
The Heart is a Lonely Hunter
In the Land of the Deaf
Johnny Belinda
The Miracle Worker - Original version with Patty Duke,
The Miracle Worker (remake) Version with Melissa Gilbert in the title role of Helen Keller.
Mr. Holland's Opus
A Summer to Remember
You should now:
Go back to Characteristics
![]() E-mail J'Anne Ellsworth
at Janne.Ellsworth@nau.edu
E-mail J'Anne Ellsworth
at Janne.Ellsworth@nau.edu
Course developed by J'Anne
Ellsworth
![]()
Copyright © 1999 Northern Arizona
University
ALL RIGHTS RESERVED