SPH405
| Neurological Foundations of Speech, Language and Hearing |
![]()
![]()
![]()
![]()
![]()
![]()
Visual System and Evaluation of Communication
GOAL: Relate the A/P of the central visual system to the evaluation of communication.
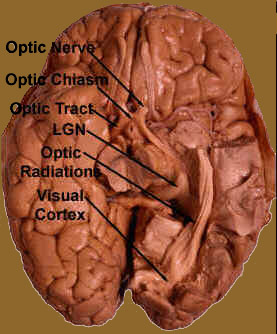
Trace the central visual system from the optic nerve to the occipital cortex (and the midbrain nuclear connections).
Demonstrate visual field screening
Relate visual field deficits to evaluation of communication disorders.
The CENTRAL visual system can be said to begin at the Thalamus.
One might question the separation of the visual system into peripheral and central sections.
Cranial nerves are supposed to be part of the peripheral nervous system. But the optic nerves are more "brain tracts" than they are "nerves" in a proper sense.
Thalamic connections begin at the LATERAL GENICULATE NUCLEUS. At thislocation are the cell bodies for the forst parts of the central optic tracts
-
Lateral geniculate neurons are arranged in a manner consistent with the retinal arrangement. In other words, the neurons are arranged like the rods and cones to which they are attached.
Fibers (axons) from the lateral geniculate nucleus fan out toward the cerebral cortex in the OPTIC RADIATION.
Disease at the Lateral Geniculate Nucleus level might result in localized (central) visual field deficits. The patient might complain of blindness on the center of the visual field, or in one or the other quadrants, and so on.
Some fibers of the optic tracts communicate directly to the Midbrain.
These synapse in two places: the SUPERIOR COLLICULUS and the PRETECTAL NUCLEUS
-
The superior colliculus:
- Action potentials for consensual tracking.
- Muscles of tracking must act in unison
- Retinal impulses play a role.
- Fusal impulses from the muscle fibers play a more important role.
- Accommodation reflex.
- Action potentials for light reflex
- If disease here, light reflex will be disrupted
- While other oculomotor reflexes will not.
- EG: consensual pupillary constriction associated with convergence.
- Impulses descend to Ocular Nucleus from the cerebral cortex.
- Oculomotor reflexes are not directly dependent upon retinal stimulation.
The Pretectal Nucleus.
No matter, all the effectors are innervated ultimately by the Oculomotor Nerve.
After the Lateral Geniculate Nucleus, most of the fibers continue on to the Visual Cortex.
First they pass through the posterior limb of the Internal Capsule
The Visual Cortex is in the Occipital Lobe.
-
The majority is in the walls of the CALCARINE SULCUS of this lobe.
- Visual fibers terminate in the lips of this sulcus.
- This is area 17
The fibers that fan out of the lateral geniculate into the lobe are known as the OPTIC RADIATION
-
One takes fibers directly into the occipital lobe.
- These are fibers from the superior retinal half.
- They terminate on the upper lip of the Calcarine Sulcus.
- This is loop of nerve fibers is called MEYER'S LOOP
- Looping fibers originate in the inferior halves of the retinae.
- These fibers terminate at the inferior lip of the Calcarine Sulcus.
- Lesions of the temporal lobe can produce visual disturbances
- Such lesions can also produce auditory disturbances.
- Hamilton doesn't mention direct fibers.

The visual field is that area of the environment the individual can see with both eyes open. Field disturbances are called ANOPSIA
Anopsia can be QUADRANTAL (1/4)
They can be hemi-(1/2)
They are HOMONYMOUS if the same portion is involved for both eyes.
They are HETERONYMOUS if opposite portions of the visual field are involved for each eye.
One screens visual fields with the confrontation test.
- Object is about halfway between examiner and patient.
- The patient signals when he/she sees the object.
- Patient should see object about the same time the examiner does.
- Damage to the optic chiasma in the center (nasal fibers cross)
- Damage to the lateral half of the chiasma would result in anopsia of the nasal field in the right eye.
- destruction of the right optic tract
- right Lateral Geniculate destruction.
- Destruction of Meyer's loop fibers in the right Temportal Lobe.
- Destruction of the inferior lip of the right Calcarine Sulcus.
- Destruction of the direct optic tracts between the lateral geniculate nucleus and the calcarine sulcus (through posterior limb of internal capsule.
- Destruction of the superior lip of the calcarine fissure.
- Damage to the inferior retina
- Damage to the lower lip of the calcarine fissure
Once you have finished you should:
Go on to Group
Assignment 1
or
Go back to Visual System
E-mail Bill Culbertson
at bill.culbertson@nau.edu
Call Bill Culbertson
at (520) 523-7440
Copyright © 1999
Northern Arizona University
ALL RIGHTS RESERVED