| ESE424 : The Class : Mild Disabilities : Behavioral/Emotional : Anxiety | |||||
Anxiety and Depression
In this lesson we will cover two types of emotional disorders that may effect the children you serve as "severely emotionally disturbed." The lesson is divided into three major parts:
As I stated in the introduction to this topic, the lesson will cover information about the definition, incidence or prevalence of the disorder, characteristics, and treatment methods.
Anxiety
Before we begin, it is important to stress that we all have some indications of anxiety. We may be irritable or distracted when we are faced with a difficult decision, an uncomfortable situation, or under pressure to complete a task under a deadline. For most of us, the anxiety we feel is a temporary condition. For some people, this is a chronic, long-lasting, and sometimes incapacitating problem.
Are you too anxious? (A self-test)
People with Anxiety Disorders (video and audio clips)
Definition and Classification
Anxiety is classified as an internalized behavior disorder. An anxiety disorder is defined as "a feeling of worry, upset, uncertainty, and fear that comes from thinking about some threat or danger" (Mosbys, 1995). This disorder is a complex pattern of behavior that includes three responses:
Phobias
One group of anxiety disorders are phobias. A phobia is an irrational, overwhelming fear of an object or event. All people have fears. It is when they become incapacitating or significantly interfere with their independent living, work, or school that they would be considered a phobia. Children with phobias will seek to avoid the situation or object that provokes their fear.
Studies conducted during the early to mid 1930s show that a number of children exhibit a large number of fears. For example, children between the ages of 2-6 reported between 4-5 fearful reactions once every 4 1/2 days. Girls tend to evidence fears more than boys. The frequency of fears generally decreases across time. Fears also change across the different age groups.
Changes in fears (phobias) across different ages (scroll about 1/2 way down the page)
Excessive fears (phobias), even if short in duration, create sufficient discomfort to interfere with functioning. Estimates of the prevalence of phobias vary with an average of 5% of youngsters exhibiting excessive amounts of worry or fear.
Types of anxiety disorders
Anxiety is not a single condition. Rather, there are a variety of different types of anxiety disorders. Some are more prevalent in younger children. Others are more common in adolescents and adults. You may encounter children who have one (or more) of the follow anxiety disorders.
Click on each link for a definition of the condition:
Social phobia is the fear of social situations. Children with this condition may miss school or show decreased participation in common school activities. Their most common concerns are embarrassment and fear of negative evaluations.
Children with social phobia may have the following complaints:
- headache
- crying
- tantrums
- freezing up in social situations
- shrinking from engaging in social interactions with unfamiliar persons
Fears arise from a number of specific situations including:
- public speaking
- writing or eating in public
- using public restrooms
- speaking to authority figures
- going to parties or social events
- informal interactions with friends, peers, or even parents
Separation Anxiety or School Refusal
Anxiety over separation from a caregiver or parent is normal in children and even young adults. It is only when the distress on separation persists beyond that which would be expected for the child's age or is so excessive that it interferes with their overall functioning that separation anxiety becomes problematic.
Separation anxiety is the most common anxiety in children. The estimates of prevalence range from 3-12% of the population. The prevalence declines steeply after early childhood. Any evidence of separation anxiety in older adolescents may be a precursor to more serious emotional disturbance.
Generalized Anxiety Disorder (GAD)
Generalized anxiety disorder is the most common anxiety disorder in childhood. The child's fears are not focused on one specific (or a small set of) objects or situations. Rather, they occur in a number of settings, with a variety of persons or events. Children seem excessively concerned with their competence and performance (requiring repeated and chronic assurances), demonstrate nervous habits (wringing hands), sleep disturbances, and often will complain of physical pain or illness.
Symptoms include:
- restlessness or a feeling of being "on the edge"
- fatigue
- difficulty in concentrating
- irritability
- muscle tension
- disturbed sleep
Studies show that GAD is present in between 2.9 - 14% of the general population. It is more common in girls than boys. The median age of onset of GAD is 10 years of age.
Panic Attacks and Panic Disorder
Many of you may be familiar with this condition after the disclosure that Donny Osmond suffered from Panic Attacks and Panic Disorder. His interviews and the subsequent media coverage of his condition has increased the awareness of this very debilitating disorder.
Signs and Symptoms of a Panic Attack
In severe cases, panic attacks will lead to the person becoming terrified of leaving their home for fear of being alone or as a way to avoid certain situations. Panic attacks are not uncommon in adolescents. An Australian sample of children found:
- 16% of children between the ages of 12-17 experienced at least one panic attack
Whitaker (1990) reports a lifetime prevalence rate of 0.6% of the general adolescent population with an increase in clinical samples to 10-15%.
Post-Traumatic Stress Disorder
There is little research about children's reactions to traumatic events. In adults, however, their reactions may involve:
- fear
- helplessness
- horror
Children may react differently showing signs of
- disorganized or
- agitated behavior
Often the person (or child) will show increased fear or anxious reactions to stimuli associated with the event. For example, 73% of the children that were involved in the bus kidnapping in Chowchilla, Washington showed fears of busses, bus drivers, and other stimuli associated with bus trips. In children these fears or anxieties may result in clingy or dependent behaviors, sleep disturbance, depressed mood, or loss of interest in preferred activities. These symptoms will decrease over time, but a significant number of children do continue to experience anxieties and fears even after months and years.
Coping strategies effect the course of a child's prognosis for overcoming trauma. Negative coping behaviors such as blaming others, screaming, avoidance) may contribute to the persistence of symptoms. More positive coping behaviors, on the other hand, are correlated with a better prognosis.
Obsessive-Compulsive Disorder
Again, the media has helped bring the problems of this disorder to light. How many of you watched "As Good as it Gets" with Jack Nicholson? If you did, you probably have a general idea of some of the problems persons with obsessive-compulsive disorder (OCD) have. I should mention that this disorder is also prevalent in persons with mental retardation and some characteristics are also part of the definition of autism.
A model of OCD (click on the elements to learn more)
OCD is known to occur in children as young as 7 years of age but the mean onset is about 10 years old. The overall prevalence of OCD in the general population is about 1.9% although many of us, after reviewing the criteria, claim to have at least some evidence of OCD tendencies.
Etiology of Anxiety Disorders
There appears to be both a biological (anxiety disorders tend to occur in families) and a psychosocial (exposure to environmental events) cause for anxiety disorders.
The current thinking is that there is a biological predisposition toward anxiety disorders (a reactivity towards certain stimuli) that is triggered by an environmental event. It is the timing of the event along with the balance of risk and resiliency factors that determines whether a person develops an anxiety disorder.
Treatment of Anxiety Disorders
Current treatment methods emphasize a combination of a medical and psychological approach to treating anxiety disorders
Integrated bio-psychological treatments have shown good results across a variety of anxiety disorders.
Depression
What does depression mean? Perhaps it is best if you hear it from someone who has suffered from depression. Click on the link below to read Jeanne's diary.
Depression refers to a "general pervasive unhappy mood." The person with depression may experience other, related problems such as:
- irritability
- loss of the experience of pleasure
- social withdrawal
- lowered self-esteem
- the inability to concentrate (may be misdiagnosed as ADHD)
- poor academic performance
- alterations of biologic functions (sleep cycles, hunger cycles, bowel problems)
- somatic complaints (headache, illness, pain)
- a conduct disorder (a later lesson)
- alcohol or substance abuse
Facts and Figures about Depression
Depression may also be "masked." That is, the features of depression are hidden by other, and sometimes paradoxical, symptoms (hyperactivity, distractibility). Young children especially will often display depression in age-related forms and ways that may be different from adult depression. It is also important to differentiate between periods of sadness and negative affect, which we all have and are much more pronounced in adolescence, and periods of true depression, which are much more long lasting and intense.
Defining Depression
But what, you say, is depression?
As you can see, there doesn't appear to be a definitive definition of depression. Rather, depression is typically identified by the symptoms it presents. The accepted view is that depression is a syndrome rather than a disorder. The link below takes you to a depression checklist. You can take the test or simply view the questions. You might, however, want to bookmark this site for your records.
A Depression Checklist (Adult symptoms)
The Epidemiology of Depression
Major depressive disorders are by far the most common form of an affective disorder among children and adolescents. Many researchers feel that the facts and figures I am about to present are underrepresentative of the true extent of the problem.
- Community surveys show that about 0.4-2.5% of children have depression, between 0.4 - 8.3% of adolescents are diagnosed as depressed
- By the age of 19, approximately 28% of adolescents will have
experienced a major depressive incident (Lewisohn, Rhode, & Seeley,
1998)
- 35% of females and 19% of males
- There is a 2:1 ration of girls to boys who report a major depressive episode
- Major reports indicate that depression is increasing
- The median age of onset is 15.5 years (most prevalent in adolescence and adulthood)
- Median duration of a depressive incident is 8 weeks (range 2-250 weeks)
- Earlier onset depression is associated with longer depressive episodes
- Depression recurs
- 5% will experience another episode within 6 months
- 12% within one year
- 33% within 4 years
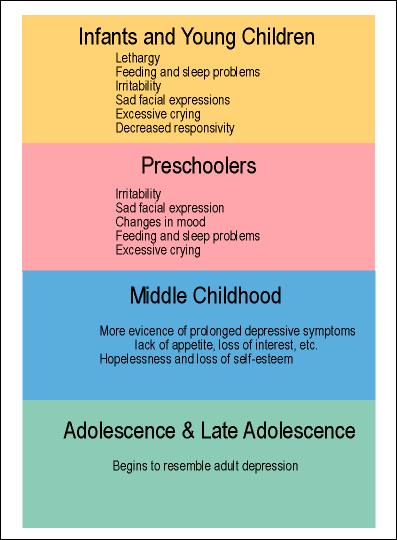
Variance in Depression by Age
Epidemiological studies show that the symptoms of depression vary by the age of the child. The symptoms displayed by a teenager vary considerably from that of a young child.
Etiology of Depression
Depression is a complex disorder and is likely caused by many factors. The three most frequently cited factors are
- Biological influences - inheritance and genetic predisposition
- Biochemistry - neurotransmitter imbalances
- Social-Psychological influences - separation and loss, learned helplessness
Etiology of Mood Disorders (Depression)
Treating Depression
Depression is a treatable condition. Although many potential treatments exist, they tend to cluster into one of two general categories:
- Psychosocial Therapies
- teaching a person to confront their maladaptive thoughts (attributions, excessively high expectations, negative self-evaluations)
- increasing pleasurable experiences
- increasing social skills
- improving communication and conflict resolution
- improving social problem solving
- Pharmacological or Medical Intervention
- antidepressant medications
- serotonin (a neurotransmitter associated with depression) reuptake inhibitors
Medications Used to Treat Depression
Enter the online lesson content here
Once you have finished you should:
Go on to Activity
3: Educational Impacts of Anxiety and Depression
or
Go back to Emotional
and Behavioral Disorders
E-mail Larry Gallagher at Larry.Gallagher@nau.edu
Copyright © 2000 Northern Arizona
University
ALL RIGHTS RESERVED